Mechanisms of Action Comparison
Retatrutide and Cagrilintide represent distinct approaches to weight management, each targeting different hormonal pathways to achieve therapeutic effects. Understanding their mechanisms of action provides crucial insights into their comparative efficacy and potential applications in clinical practice.
Retatrutide operates as a triple hormone receptor agonist, simultaneously activating three key receptors: glucagon-like peptide-1 (GLP-1), glucose-dependent insulinotropic polypeptide (GIP), and glucagon. This multifaceted approach creates a comprehensive metabolic intervention that addresses multiple aspects of appetite regulation and energy expenditure. The GLP-1 receptor activation enhances insulin secretion, suppresses glucagon release, and slows gastric emptying, while GIP receptor stimulation further amplifies insulin response and promotes glucose uptake in peripheral tissues. The glucagon receptor activation increases energy expenditure through enhanced lipolysis and thermogenesis, creating a synergistic effect that maximises weight loss potential.
Cagrilintide functions as a long-acting amylin analogue, mimicking the effects of the naturally occurring hormone amylin. This peptide hormone plays a crucial role in satiety signalling and metabolic regulation through its actions on the central nervous system. By binding to amylin receptors in the brain, particularly in the hypothalamus, Cagrilintide promotes feelings of fullness and reduces food intake. The mechanism involves slowing gastric emptying, which prolongs the sensation of satiety and reduces overall caloric consumption. Additionally, amylin receptor activation influences glucose metabolism and insulin sensitivity, contributing to improved metabolic outcomes beyond weight management alone.
Ready to Order?
Choose your preferred amount below, fast shipping and secure checkout.
-
Reta 10mg 3 Vials
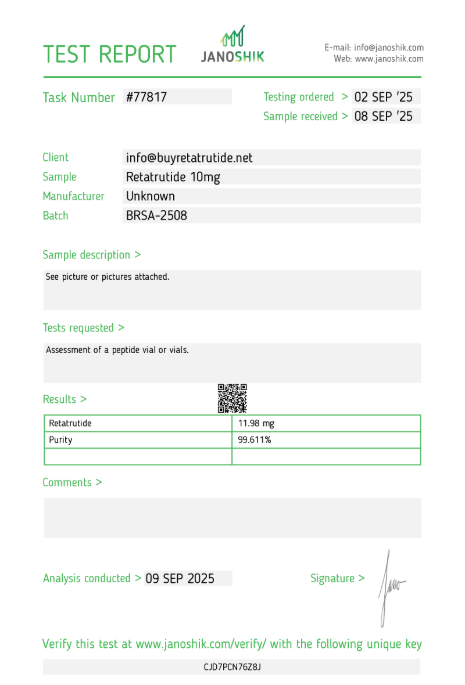
£195.00Independently verified COA. UK stock, worldwide delivery. For lab use only.
The fundamental difference between these mechanisms lies in their scope of action. Retatrutide’s triple agonist approach provides comprehensive coverage of multiple metabolic pathways simultaneously, potentially offering more robust and sustained effects. In contrast, Cagrilintide’s targeted amylin receptor activation focuses specifically on appetite regulation and satiety enhancement, which may provide more predictable and manageable side effect profiles. Both approaches represent significant advances in investigational tri-agonists for weight management, but their distinct mechanisms suggest different optimal applications and patient populations.
Preclinical studies have demonstrated that Retatrutide’s multi-receptor activation creates additive effects that exceed the sum of individual receptor stimulation. The simultaneous activation of GLP-1, GIP, and glucagon receptors appears to create synergistic interactions that enhance both weight loss and metabolic improvements. Cagrilintide’s amylin receptor targeting, while more focused, has shown remarkable efficacy when combined with other agents, particularly GLP-1 receptor agonists like semaglutide, suggesting potential for combination therapy approaches.
The pharmacokinetic profiles of these agents also differ significantly. Retatrutide’s triple receptor activation requires careful dosing optimisation to balance efficacy with tolerability, as simultaneous activation of multiple pathways may increase the risk of adverse effects. Cagrilintide’s more targeted approach may offer better tolerability profiles, particularly in patients who experience significant gastrointestinal side effects with multi-receptor agonists. These mechanistic differences inform clinical decision-making and help healthcare providers select the most appropriate therapy for individual patients based on their specific needs and tolerability profiles.
Clinical Efficacy and Results
Clinical trial data for both Retatrutide and Cagrilintide demonstrate significant weight loss efficacy, though through different therapeutic approaches. Phase II trials have provided compelling evidence for both agents, establishing their potential as effective treatments for obesity and related metabolic disorders.
Retatrutide has shown remarkable efficacy in clinical trials, with Phase II data demonstrating up to 24% body weight reduction over 48 weeks in adults with obesity without diabetes. This represents one of the highest weight loss percentages reported for any single-agent therapy in clinical trials. The weight loss was achieved gradually and sustained throughout the study period, with participants maintaining significant reductions even at the 48-week endpoint. Beyond weight loss, Retatrutide demonstrated substantial improvements in metabolic parameters, including reductions in fasting glucose levels, improvements in insulin sensitivity, and favourable changes in lipid profiles. These comprehensive metabolic benefits position Retatrutide as a potential game-changer in obesity treatment.
Cagrilintide has demonstrated impressive efficacy both as monotherapy and in combination approaches. As a standalone therapy, participants receiving 4.5 mg weekly achieved an average weight loss of 10.8% over 26 weeks, compared to 3% in the placebo group. This represents a clinically meaningful difference that exceeds the efficacy of many currently available weight management medications. The weight loss was accompanied by improvements in glycemic control, with significant reductions in HbA1c levels, suggesting potential benefits for patients with both obesity and diabetes.
The combination of Cagrilintide with semaglutide, known as CagriSema, has shown particularly promising results. Clinical trials have demonstrated over 20% average weight loss with this combination approach, approaching the efficacy observed with Retatrutide monotherapy. This suggests that targeted combination therapy may provide comparable efficacy to triple receptor agonists while potentially offering better tolerability profiles. The additive effects of amylin and GLP-1 receptor activation create synergistic benefits that exceed either agent alone.
Comparative efficacy data reveals interesting patterns in patient response. Retatrutide’s triple receptor activation appears to provide more comprehensive metabolic benefits, with improvements extending beyond weight loss to include significant enhancements in insulin sensitivity and glucose metabolism. Cagrilintide’s focused approach on appetite regulation results in more predictable weight loss patterns, with fewer fluctuations in efficacy over time. Both agents have shown the ability to maintain weight loss over extended periods, addressing a critical challenge in obesity treatment.
Patient population differences may influence the relative efficacy of these agents. Retatrutide appears particularly effective in patients with significant insulin resistance and metabolic dysfunction, where its comprehensive receptor activation provides maximal benefit. Cagrilintide may be more suitable for patients who require focused appetite control and have experienced gastrointestinal intolerance with other weight management medications. The clinical trial data suggests that both agents can achieve substantial weight loss, but optimal patient selection may maximise their therapeutic potential.
Safety Profiles and Side Effects
Safety considerations play a crucial role in evaluating the clinical utility of both Retatrutide and Cagrilintide. Understanding their adverse event profiles helps healthcare providers make informed decisions about patient selection and monitoring requirements. Both agents have demonstrated generally favourable safety profiles in clinical trials, though their side effect patterns differ based on their distinct mechanisms of action.
Retatrutide’s safety profile reflects its triple receptor activation approach, with gastrointestinal symptoms being the most commonly reported adverse events. Nausea, diarrhoea, vomiting, and constipation occur frequently, particularly during the initial treatment period. These symptoms are typically mild to moderate in severity and tend to diminish over time as patients adjust to the medication. The gastrointestinal side effects are consistent with GLP-1 receptor activation and are generally manageable with appropriate dosing strategies and patient education. More serious adverse events are rare but can include pancreatitis, gallbladder disease, and hypoglycaemia, particularly in patients with diabetes.
Cagrilintide has demonstrated a favourable safety profile with generally mild adverse events. The most common side effects include nausea and constipation, which are typically mild to moderate in severity. The overall discontinuation rate due to adverse events is approximately 10%, suggesting good tolerability for most patients. When used in combination with semaglutide, the incidence of side effects does not appear to increase significantly compared to either agent alone, indicating that the combination approach maintains acceptable safety margins. The focused amylin receptor activation appears to result in fewer systemic side effects compared to multi-receptor agonists.
Comparative safety data reveals important differences between these agents. Retatrutide’s comprehensive receptor activation may result in more frequent gastrointestinal side effects, particularly during the initial treatment period. However, these effects are generally predictable and manageable with appropriate patient counselling and dose titration. Cagrilintide’s more targeted approach appears to offer better tolerability, particularly for patients who have experienced significant gastrointestinal intolerance with other weight management medications. The amylin receptor targeting seems to provide effective appetite control with fewer systemic side effects.
Long-term safety considerations remain important for both agents. Retatrutide’s triple receptor activation requires ongoing monitoring for potential effects on multiple organ systems, including the pancreas, gallbladder, and cardiovascular system. Cagrilintide’s focused mechanism may offer advantages in long-term safety, though comprehensive long-term data is still being collected. Both agents require careful patient selection and monitoring, particularly in patients with pre-existing medical conditions that may be affected by their mechanisms of action.
Patient-specific factors significantly influence the safety profiles of these agents. Retatrutide may be more suitable for patients who can tolerate initial gastrointestinal side effects in exchange for potentially greater weight loss efficacy. Cagrilintide may be preferable for patients who require effective appetite control with minimal systemic side effects. The safety profiles of both agents support their potential as valuable additions to the obesity treatment armamentarium, with appropriate patient selection and monitoring being key to optimising their therapeutic benefits while minimising risks.
Regulatory Status and Availability
The regulatory landscape for both Retatrutide and Cagrilintide reflects their status as investigational compounds in advanced clinical development. Understanding their current regulatory positions provides insight into their potential timeline for clinical availability and the regulatory considerations that will influence their market introduction.
Retatrutide is currently undergoing Phase III clinical trials, representing the final stage of clinical development before potential regulatory approval. The compound has progressed through Phase I and Phase II trials with promising results, demonstrating both efficacy and safety in multiple patient populations. The Phase III programme is designed to confirm the efficacy and safety findings from earlier trials in larger, more diverse patient populations. Regulatory submissions are anticipated following successful completion of the Phase III trials, with potential approval timelines dependent on the specific regulatory pathways pursued in different jurisdictions.
Cagrilintide has also advanced to Phase III clinical development through Novo Nordisk’s REDEFINE programme. This comprehensive clinical development programme is evaluating the efficacy and safety of Cagrilintide in individuals with obesity or overweight conditions. The programme includes multiple studies designed to assess both monotherapy and combination therapy approaches, reflecting the compound’s potential for flexible clinical application. The Phase III trials are expected to provide definitive evidence of Cagrilintide’s clinical utility and safety profile.
Regulatory considerations for both agents include the evaluation of their risk-benefit profiles, particularly given their novel mechanisms of action. Retatrutide’s triple receptor activation approach represents a significant advancement in obesity treatment, but also introduces regulatory complexity due to its comprehensive mechanism. Cagrilintide’s focused amylin receptor targeting may offer regulatory advantages through its more predictable mechanism and potentially favourable safety profile. Both agents will require comprehensive safety databases and long-term follow-up data to support regulatory approval.
Market availability timelines for both compounds remain subject to successful completion of Phase III trials and regulatory approval processes. Retatrutide’s development timeline suggests potential availability within the next few years, assuming successful trial completion and regulatory approval. Cagrilintide’s development through Novo Nordisk’s established infrastructure may facilitate more rapid progression through regulatory processes. Both agents represent significant advances in obesity treatment and are likely to receive priority review consideration from regulatory authorities.
The regulatory pathway for these investigational compounds will likely include specific requirements for post-marketing surveillance and long-term safety monitoring. Given their novel mechanisms of action and the chronic nature of obesity treatment, regulatory authorities will require comprehensive safety databases and ongoing monitoring programmes. These requirements reflect the importance of ensuring patient safety while providing access to potentially transformative treatments for obesity and related metabolic disorders.
Head-to-Head Comparison
Direct comparison between Retatrutide and Cagrilintide reveals distinct advantages and considerations for each agent. While head-to-head clinical trials are limited, available data provides valuable insights into their relative efficacy, safety, and clinical utility. Understanding these comparative aspects helps healthcare providers make informed decisions about optimal therapy selection for individual patients.
Efficacy comparisons demonstrate that Retatrutide achieves superior weight loss as monotherapy, with up to 24% body weight reduction compared to Cagrilintide’s 10.8% reduction. However, this comparison must be interpreted cautiously given differences in study duration and patient populations. Retatrutide’s triple receptor activation provides comprehensive metabolic benefits beyond weight loss, including significant improvements in insulin sensitivity and glucose metabolism. Cagrilintide’s focused amylin receptor targeting offers more predictable appetite control with potentially better tolerability profiles.
Safety comparisons reveal important differences in side effect profiles. Retatrutide’s comprehensive receptor activation results in more frequent gastrointestinal side effects, particularly during the initial treatment period. Cagrilintide’s targeted approach appears to offer better tolerability, with lower rates of gastrointestinal adverse events. The discontinuation rate for Cagrilintide is approximately 10%, suggesting good overall tolerability. Retatrutide’s side effect profile, while manageable, may require more careful patient selection and monitoring.
Combination therapy potential represents a significant advantage for Cagrilintide. When combined with semaglutide, Cagrilintide achieves over 20% weight loss, approaching the efficacy of Retatrutide monotherapy. This suggests that targeted combination approaches may provide comparable efficacy with potentially better tolerability. Retatrutide’s comprehensive mechanism may limit its combination potential, as additional receptor activation could increase side effect risks without proportional efficacy gains.
Patient selection considerations favour different agents for different populations. Retatrutide may be optimal for patients with significant insulin resistance and metabolic dysfunction, where its comprehensive receptor activation provides maximal benefit. Cagrilintide may be preferable for patients who require effective appetite control with minimal systemic side effects, particularly those who have experienced gastrointestinal intolerance with other weight management medications. The choice between these agents should be individualised based on patient characteristics and treatment goals.
Long-term considerations suggest different advantages for each agent. Retatrutide’s comprehensive metabolic effects may provide sustained benefits beyond weight loss, potentially addressing multiple aspects of metabolic syndrome. Cagrilintide’s focused approach may offer advantages in long-term safety and tolerability, though comprehensive long-term data is still being collected for both agents. The optimal choice may depend on individual patient priorities regarding efficacy versus tolerability.
Clinical Trial Limitations
Understanding the limitations of clinical trial data is crucial for interpreting the comparative efficacy and safety of Retatrutide and Cagrilintide. While both agents have demonstrated promising results in clinical trials, several factors limit the generalisability of these findings and highlight the need for continued research and clinical evaluation.
Study design variations significantly impact the comparability of clinical trial results between Retatrutide and Cagrilintide. Retatrutide trials have typically employed longer study durations, with some extending to 48 weeks, while Cagrilintide trials have often used shorter durations, typically around 26 weeks. These differences in study length make direct efficacy comparisons challenging, as weight loss patterns may differ over time. Additionally, patient population characteristics vary between studies, including differences in baseline body mass index, age, gender distribution, and presence of comorbidities such as diabetes.
Dosing regimen differences further complicate comparative analysis. Retatrutide trials have explored various dosing strategies, with optimal dosing still being determined through ongoing research. Cagrilintide trials have primarily focused on weekly dosing regimens, but optimal dosing for both agents remains subject to ongoing investigation. These dosing variations may influence both efficacy and safety outcomes, making it difficult to establish definitive comparative profiles.
Patient selection criteria create additional limitations in generalising trial results to broader clinical populations. Clinical trials typically employ strict inclusion and exclusion criteria that may not reflect real-world patient populations. Patients with significant comorbidities, those taking multiple medications, or those with complex medical histories may be underrepresented in clinical trials. This limits the applicability of trial results to diverse clinical settings where patients often present with multiple health conditions.
Long-term safety and efficacy data remain limited for both agents, as most clinical trials have been of relatively short duration. Obesity is a chronic condition requiring long-term management, and the sustainability of weight loss and long-term safety profiles beyond the trial periods remain uncertain. Extended follow-up studies are needed to establish the durability of treatment effects and identify any long-term safety concerns that may not be apparent in shorter-term trials.
Real-world effectiveness may differ from clinical trial efficacy due to various factors including patient adherence, healthcare provider experience, and practical implementation challenges. Clinical trials provide controlled environments with close monitoring and support, which may not be replicable in routine clinical practice. The gap between clinical trial efficacy and real-world effectiveness represents an important consideration for healthcare providers and patients.
Related Research Comparisons
The landscape of obesity treatment continues to evolve with multiple investigational compounds targeting different pathways. Understanding how Retatrutide and Cagrilintide compare to other emerging therapies provides valuable context for their potential clinical applications and helps identify optimal treatment strategies for different patient populations.
Combination therapy approaches represent a significant area of research interest, particularly for Cagrilintide. The Retatrutide vs CagriSema comparison highlights the potential of combining amylin and GLP-1 receptor agonists. CagriSema, which combines Cagrilintide with semaglutide, has demonstrated over 20% weight loss in clinical trials, approaching the efficacy of Retatrutide monotherapy. This suggests that targeted combination approaches may provide comparable efficacy with potentially better tolerability profiles than comprehensive single-agent therapies.
Other experimental compounds offer additional insights into the evolving landscape of obesity treatment. The Retatrutide vs Amycretin comparison explores another novel amylin-based approach, while the Retatrutide vs Orforglipron analysis examines oral GLP-1 receptor agonists. The Retatrutide vs Danuglipron comparison evaluates small molecule GLP-1 agonists, and the Retatrutide vs VK2735 analysis explores GIP receptor antagonists. These comparisons highlight the diverse approaches being investigated for obesity treatment.
Multi-receptor agonist comparisons provide valuable context for Retatrutide’s position in the treatment landscape. The Retatrutide vs Tirzepatide comparison examines dual GLP-1/GIP receptor agonists, while the Retatrutide vs Pemvidutide analysis explores GLP-1/glucagon dual agonists. These comparisons demonstrate the progression from single-receptor to multi-receptor approaches, with Retatrutide representing the most comprehensive triple agonist currently in development.
Established GLP-1 receptor agonists provide important benchmarks for evaluating newer therapies. The Retatrutide vs Semaglutide comparison highlights the significant advances achieved with newer multi-receptor approaches compared to established GLP-1 mono-agonists. Similarly, comparisons with Retatrutide vs Contrave demonstrate the evolution from central appetite control mechanisms to targeted hormonal approaches.
Future research directions continue to explore novel mechanisms and combination approaches. The Retatrutide vs Maridebart comparison examines another investigational metabolic compound, while ongoing research explores additional combination therapies and novel targets. These comparisons highlight the dynamic nature of obesity treatment research and the potential for continued innovation in this field.
Frequently Asked Questions
General Questions
- What is the main difference between Retatrutide and Cagrilintide?
Retatrutide is a triple hormone receptor agonist that simultaneously activates GLP-1, GIP, and glucagon receptors, while Cagrilintide is an amylin receptor agonist that specifically targets appetite regulation and satiety enhancement. - Which agent provides better weight loss results?
Retatrutide achieves superior weight loss as monotherapy with up to 24% body weight reduction, while Cagrilintide achieves 10.8% weight loss alone but can reach over 20% when combined with semaglutide. - Are both agents currently available for clinical use?
Both Retatrutide and Cagrilintide are investigational compounds currently undergoing Phase III clinical trials and are not yet approved for clinical use.
Mechanism Questions
- How does Retatrutide’s triple receptor activation work?
Retatrutide simultaneously activates GLP-1, GIP, and glucagon receptors, creating synergistic effects that enhance insulin secretion, suppress appetite, slow gastric emptying, and increase energy expenditure. - What makes Cagrilintide’s mechanism unique?
Cagrilintide mimics the hormone amylin, binding to amylin receptors in the brain to promote feelings of fullness, reduce food intake, and slow gastric emptying for prolonged satiety. - Can these agents be used together?
While both agents target different pathways, their combination has not been extensively studied and may increase side effect risks without proportional efficacy gains.
Safety Questions
- What are the most common side effects of Retatrutide?
The most common side effects include gastrointestinal symptoms such as nausea, diarrhoea, vomiting, and constipation, which are typically mild to moderate and diminish over time. - How does Cagrilintide’s safety profile compare?
Cagrilintide generally has a more favourable safety profile with lower rates of gastrointestinal side effects, though nausea and constipation can still occur. - Are there any serious safety concerns with either agent?
Both agents have demonstrated generally favourable safety profiles in clinical trials, though long-term safety data remains limited and ongoing monitoring is required.
Clinical Questions
- Which patients might benefit most from Retatrutide?
Retatrutide may be optimal for patients with significant insulin resistance and metabolic dysfunction who can tolerate initial gastrointestinal side effects for potentially greater weight loss efficacy. - Who might be better suited for Cagrilintide?
Cagrilintide may be preferable for patients who require effective appetite control with minimal systemic side effects, particularly those with gastrointestinal intolerance to other weight management medications. - What is the expected timeline for clinical availability?
Both agents are in Phase III trials with potential availability within the next few years, assuming successful trial completion and regulatory approval.
Order Retatrutide Online
Available in 10mg vials. Select your pack size and checkout securely below.
-
Reta 10mg 3 Vials
£195.00Independently verified COA. UK stock, worldwide delivery. For lab use only.
Conclusion
The comparison between Retatrutide and Cagrilintide highlights the evolving landscape of obesity treatment, with both agents representing significant advances in therapeutic approaches. Retatrutide’s triple receptor activation offers comprehensive metabolic benefits with superior weight loss efficacy, while Cagrilintide’s focused amylin receptor targeting provides effective appetite control with potentially better tolerability profiles.
Clinical trial data demonstrates that both agents can achieve substantial weight loss, with Retatrutide achieving up to 24% body weight reduction and Cagrilintide reaching over 20% when combined with semaglutide. The choice between these agents should be individualised based on patient characteristics, tolerability considerations, and treatment goals. Retatrutide may be optimal for patients with significant metabolic dysfunction, while Cagrilintide may be preferable for those requiring focused appetite control with minimal side effects.
As both agents progress through Phase III clinical trials, continued research will provide additional insights into their long-term safety and efficacy profiles. The potential for combination therapy approaches, particularly with Cagrilintide, suggests exciting possibilities for optimising obesity treatment outcomes. Healthcare providers and patients should stay informed about the latest developments in this rapidly evolving field as these investigational compounds move closer to clinical availability.
For concentration calculations, visit our research calculator. For handling guidelines, see our information hub. Find verified suppliers for Cagrilintide and Retatrutide research materials with COA documentation.
For laboratory research use only. Not for human consumption. No medical advice. Information relevant to the United Kingdom.