Mechanisms of Action
Understanding the distinct mechanisms of action between Retatrutide and Amycretin reveals why these investigational compounds represent fundamentally different approaches to weight management and metabolic control. While both target appetite regulation and glucose metabolism, their molecular strategies create unique therapeutic profiles with different advantages and limitations.
Retatrutide operates as a tri-agonist targeting GLP-1, GIP, and glucagon receptors, representing a single-molecule approach to multi-receptor activation. This comprehensive mechanism allows simultaneous activation of three distinct hormonal pathways, each contributing to different aspects of metabolic regulation. The GLP-1 component slows gastric emptying, promotes satiety, and enhances insulin secretion, while GIP activation improves insulin sensitivity and glucose metabolism. The glucagon component increases energy expenditure and promotes fat oxidation, creating a synergistic effect that addresses multiple aspects of metabolic dysfunction simultaneously.
Amycretin, developed by Novo Nordisk, employs a dual agonist approach, combining GLP-1 and amylin receptor activation in a single molecule. This strategy focuses on two complementary pathways that work synergistically to enhance appetite control and promote satiety. The GLP-1 component provides the established benefits of insulin secretion enhancement and appetite suppression, while the amylin component adds additional gastric emptying delay and satiety promotion through different mechanisms. This dual targeting creates a streamlined approach that may offer better tolerability compared to triple agonist compounds.
The key difference lies in their therapeutic strategy: Retatrutide’s comprehensive triple agonist approach versus Amycretin’s focused dual agonist mechanism. Retatrutide’s approach may provide more extensive metabolic benefits through glucagon receptor activation, which increases energy expenditure and promotes fat burning. Amycretin’s dual agonist approach may offer better tolerability and potentially fewer side effects due to its more focused receptor targeting, while still providing significant weight loss benefits.
Both approaches represent significant advances beyond single-receptor agonists, addressing multiple aspects of metabolic dysfunction that contribute to obesity and type 2 diabetes. The choice between these mechanisms may ultimately depend on individual patient characteristics, including baseline metabolic profile, comorbidities, and tolerance for potential side effects.
Ready to Order?
Choose your preferred amount below, fast shipping and secure checkout.
-
Reta 10mg 3 Vials
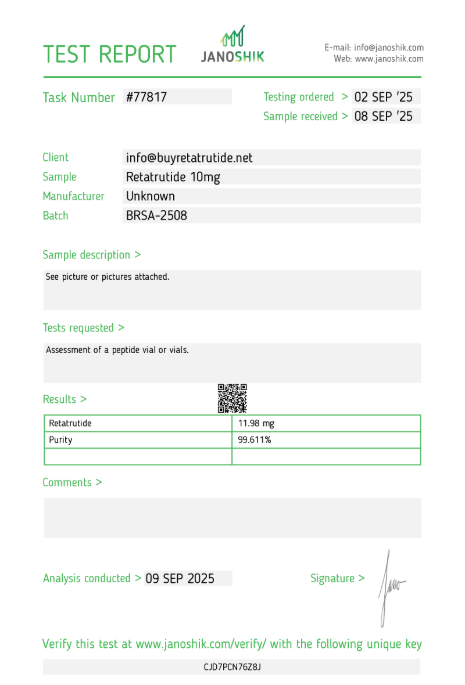
£195.00Independently verified COA. UK stock, worldwide delivery. For lab use only.
Clinical Efficacy & Weight Loss Results
Clinical trial data provides compelling evidence for both compounds’ effectiveness in weight management, though with notable differences in magnitude, duration, and patient populations studied. The results highlight the potential advantages of multi-receptor targeting versus dual agonist approaches in achieving significant weight loss and metabolic improvements.
Retatrutide has demonstrated exceptional weight loss results in clinical trials. In a Phase 2 study, participants receiving the highest dose (12 mg) experienced an average weight reduction of 24.2% after 48 weeks. These results are particularly remarkable because they approach the efficacy of certain bariatric surgical procedures while being achieved through pharmacological intervention. The weight loss appears to be sustained and progressive, with participants continuing to lose weight throughout the treatment period. Additionally, Retatrutide has shown significant improvements in metabolic markers, including HbA1c reduction and lipid profile improvements.
Amycretin has shown impressive results in early clinical trials, demonstrating substantial weight loss across different administration routes. In a Phase 1 trial involving oral administration, participants receiving 100 mg per day achieved a mean weight loss of 13.1% over 12 weeks, compared to 1.2% in the placebo group. More impressively, in a Phase 1b/2a trial assessing subcutaneous administration, participants receiving a 60 mg dose over 36 weeks experienced a 24.3% reduction in body weight, compared to a 1.1% reduction in the placebo group. These findings highlight Amycretin’s potential as a highly effective weight management therapy.
Studies evaluating the weight-loss outcomes of both compounds have shown promising results in preclinical and early clinical trials. Both compounds have demonstrated significant reductions in body weight compared to placebo, with Retatrutide showing slightly superior efficacy in some studies. The mechanisms of action of these multi-agonist compounds involve the modulation of appetite, energy expenditure, and glucose metabolism, leading to improved weight loss outcomes. However, direct head-to-head comparisons between Retatrutide and Amycretin are limited, making it challenging to draw definitive conclusions about their comparative efficacy in weight management.
The clinical data suggests that while Retatrutide may offer superior weight loss efficacy based on available data, Amycretin provides a valuable alternative with potentially better tolerability due to its dual agonist approach. The choice between these compounds may depend on individual patient characteristics, including baseline weight, comorbidities, diabetes status, and tolerance for potential side effects.
Safety Profiles & Side Effects
Safety evaluation remains crucial for both compounds, as their different mechanisms of action create distinct adverse event profiles that influence their suitability for different patient populations. Understanding these safety considerations helps researchers and clinicians make informed decisions about their potential therapeutic applications.
Retatrutide, as a tri-agonist targeting multiple receptors, may have a broader spectrum of side effects compared to single-receptor agonists or dual agonist compounds. Common adverse events associated with Retatrutide include gastrointestinal symptoms such as nausea, vomiting, and diarrhoea, which are typical of agents targeting GLP-1 receptors. The triple agonist mechanism may also contribute to additional metabolic effects, including potential sleep disturbances and increased heart rate at higher doses. Early clinical data suggests that these effects are generally manageable with appropriate dose titration, though the investigational status of Retatrutide means that comprehensive long-term safety data is still emerging.
Amycretin has demonstrated generally favourable safety profiles in early clinical trials, with adverse events primarily consisting of mild to moderate gastrointestinal symptoms typical of GLP-1 receptor agonists and amylin analogues. The most common treatment-emergent adverse events (TEAEs) associated with Amycretin were gastrointestinal in nature, including nausea and vomiting, which were generally mild to moderate and exhibited a dose-dependent increase in frequency. Importantly, no deaths were reported during the studies, indicating a favourable safety profile. The dual agonist approach may offer better tolerability compared to triple agonist compounds due to its more focused receptor targeting.
Both compounds share common gastrointestinal side effects typical of GLP-1 receptor agonists, including nausea, vomiting, diarrhoea, and constipation. These effects are generally mild to moderate in severity and tend to diminish over time as patients adapt to treatment. The amylin component in Amycretin may contribute to additional gastrointestinal effects, though current data suggests these are generally manageable and do not significantly impact treatment continuation rates.
Understanding the tolerability of these compounds is crucial for assessing their overall safety and feasibility for long-term use in weight management. While both drugs show promise, their investigational status means that comprehensive safety data will continue to emerge as clinical trials progress. Researchers must remain vigilant for any additional side effects or interactions that may become apparent in larger, longer-term studies, particularly regarding cardiovascular outcomes and rare adverse events.
Regulatory Status & Availability
The regulatory landscape for both compounds reflects their investigational status and the complex approval process for new weight loss medications. Understanding their current status helps set realistic expectations for potential availability and informs research planning and patient counselling.
Retatrutide is currently progressing through Phase 3 clinical trials, representing the final stage before potential regulatory approval. The compound has shown promising results in earlier phases, with Phase 2 data demonstrating significant weight loss and metabolic benefits. If ongoing Phase 3 trials confirm these findings and establish long-term safety, regulatory approval could potentially occur around 2026. The development timeline suggests that Retatrutide may be among the first triple agonist weight loss medications to reach the market, representing a significant advancement in obesity pharmacotherapy.
Amycretin’s regulatory pathway differs significantly, with development led by Novo Nordisk. Based on the promising results from early-phase trials, Novo Nordisk plans to advance both subcutaneous and oral formulations of Amycretin into Phase 3 clinical development for weight management. These trials are expected to commence in early 2026, suggesting a potential approval timeline similar to Retatrutide. The compound’s dual agonist approach and favourable safety profile may accelerate the regulatory review process compared to more complex triple agonist compounds.
Both compounds face regulatory challenges common to weight loss medications, including requirements for comprehensive safety data, particularly regarding cardiovascular outcomes. The investigational nature of these drugs means that regulatory agencies will require extensive evidence of both efficacy and safety before approval. This cautious approach reflects lessons learned from previous weight loss medications that were withdrawn due to safety concerns, emphasising the importance of thorough evaluation.
The current regulatory status means that neither compound is available for clinical use outside of research settings. Patients and healthcare providers must wait for completion of clinical trials and regulatory review before these medications become accessible. This timeline underscores the importance of managing expectations while these promising compounds progress through the development pipeline, and highlights the need for continued research into alternative treatment options for patients with obesity and related metabolic conditions.
Head-to-Head Comparison
Direct comparison of Retatrutide and Amycretin reveals distinct advantages and limitations for each compound, highlighting the different therapeutic strategies employed by these investigational treatments. Understanding these differences helps researchers and clinicians evaluate their potential therapeutic roles and suitability for different patient populations.
Retatrutide’s triple agonist mechanism appears to offer superior weight loss efficacy, with clinical trial data showing up to 24.2% weight reduction after 48 weeks. This performance approaches the efficacy of certain bariatric surgical procedures and represents a significant advancement in pharmacological weight management. The comprehensive receptor targeting may also provide additional metabolic benefits, particularly for patients with type 2 diabetes or metabolic syndrome. The single-molecule approach ensures consistent receptor activation ratios and may result in more predictable pharmacokinetic profiles.
Amycretin’s dual agonist approach, while targeting fewer receptors, may offer distinct advantages due to its focused mechanism and potentially better tolerability profile. The compound has demonstrated impressive weight loss results, with up to 24.3% weight reduction over 36 weeks in subcutaneous administration studies. The dual agonist mechanism may provide better tolerability compared to triple agonist compounds, potentially resulting in higher treatment adherence and better long-term outcomes. Additionally, Amycretin’s development by Novo Nordisk suggests potential advantages in formulation and delivery mechanisms.
From a mechanistic perspective, Retatrutide’s inclusion of GIP and glucagon receptor activation may provide additional benefits beyond appetite suppression and energy expenditure. GIP has been shown to enhance insulin sensitivity and glucose metabolism, while glucagon activation promotes fat oxidation and increases energy expenditure. Amycretin’s focus on GLP-1 and amylin receptors provides a more streamlined approach that may result in fewer metabolic interactions and potentially better tolerability.
The choice between these compounds may ultimately depend on individual patient characteristics and treatment goals. Patients seeking maximum weight loss may benefit from Retatrutide’s triple agonist approach, while those prioritising tolerability and potentially better adherence may prefer Amycretin’s dual agonist mechanism. Both compounds represent significant advances in obesity pharmacotherapy and offer hope for patients struggling with weight management, though their different mechanisms and safety profiles may allow for personalised treatment approaches based on individual patient needs.
Clinical Trial Limitations
Interpreting the clinical data for both compounds requires careful consideration of study limitations and methodological differences. Understanding these constraints helps researchers and clinicians make informed decisions about their potential therapeutic applications and avoid overinterpreting preliminary results.
Cross-trial comparisons between Retatrutide and Amycretin are inherently limited by differences in study design, patient populations, and treatment durations. Retatrutide’s most impressive results come from a 48-week Phase 2 study, while Amycretin’s data primarily reflects earlier-stage trials with shorter durations and different administration routes. These temporal and methodological differences make direct efficacy comparisons challenging and may underestimate either compound’s potential with longer treatment periods or different formulations.
Patient population differences also complicate comparisons between the compounds. Studies have enrolled participants with varying baseline characteristics, including different starting weights, metabolic profiles, and comorbidities. These differences can significantly influence treatment outcomes and make it difficult to determine whether observed differences reflect true drug effects or patient population characteristics. The lack of head-to-head trials means that direct comparisons must rely on cross-trial analyses, which are inherently less reliable than randomised controlled trials.
Dosing regimens vary significantly between studies, with different titration schedules and maximum doses evaluated. These differences can impact both efficacy and safety outcomes, making it challenging to determine optimal dosing strategies for either compound. The investigational nature of both drugs means that optimal dosing has not yet been established, and current regimens may not represent the final approved dosing strategies.
Long-term safety data remains limited for both compounds, as most studies have focused on shorter-term outcomes. The potential for rare or delayed adverse events requires longer follow-up periods to fully characterise. Additionally, the investigational status of both compounds means that real-world safety data is not yet available, limiting understanding of their performance in routine clinical practice. Researchers must exercise caution when extrapolating findings from clinical trials to broader patient populations, as the controlled nature of clinical studies may not reflect real-world conditions where patients may have different adherence patterns, comorbidities, or concurrent medications.
Related Research Comparisons
Understanding how Retatrutide and Amycretin compare to other investigational compounds provides valuable context for their potential therapeutic roles. These comparisons help researchers identify the unique advantages and limitations of each approach within the broader landscape of obesity pharmacotherapy.
Other Experimental Compounds
- Retatrutide vs CagriSema – Combination therapy research analysis
- Retatrutide vs Cagrilintide – Amylin analogue peptide comparison
- Retatrutide vs Orforglipron – Oral GLP-1 agonist research
- Retatrutide vs Danuglipron – Small molecule GLP-1 analysis
- Retatrutide vs VK2735 – GIP antagonist mechanism comparison
- Retatrutide vs Maridebart – Novel peptide research
- Retatrutide vs Cafraglutide – Investigational dual agonist
Multi-Receptor Agonists
- Retatrutide vs Tirzepatide – Approved dual receptor agonist
- Retatrutide vs Cotadutide – Triple receptor agonist comparison
Compare with Other Categories
- Retatrutide vs Semaglutide – Leading GLP-1 mono-agonist
- Retatrutide vs Qsymia – Combination therapy approach
Navigate Research Categories
← All Comparisons | ← Experimental Compounds
For concentration calculations, visit our research calculator. For handling guidelines, see our information hub.
Research Supplies
Find verified suppliers for Amycretin and Retatrutide research materials with COA documentation.
Order Retatrutide Online
Available in 10mg vials. Select your pack size and checkout securely below.
-
Reta 10mg 3 Vials
£195.00Independently verified COA. UK stock, worldwide delivery. For lab use only.
Frequently Asked Questions
General Questions
- What is the main difference between Retatrutide and Amycretin?
Retatrutide is a triple agonist targeting GLP-1, GIP, and glucagon receptors, while Amycretin is a dual agonist targeting GLP-1 and amylin receptors. This difference in receptor targeting may influence their efficacy and side effect profiles. - Are Retatrutide and Amycretin currently available for clinical use?
Neither compound is currently approved for clinical use. Retatrutide is in Phase 3 trials with potential approval around 2026, while Amycretin is advancing to Phase 3 trials in early 2026. - Which compound has shown better weight loss results?
Both compounds have demonstrated impressive weight loss results. Retatrutide showed up to 24.2% weight reduction after 48 weeks, while Amycretin achieved up to 24.3% weight reduction over 36 weeks in subcutaneous studies.
Mechanism Questions
- How do Retatrutide and Amycretin work?
Retatrutide activates GLP-1, GIP, and glucagon receptors simultaneously, providing comprehensive metabolic control. Amycretin activates GLP-1 and amylin receptors, offering a more focused approach to appetite regulation and satiety. - What advantages does the triple agonist approach provide?
Triple agonist mechanisms provide comprehensive metabolic control by addressing appetite regulation, insulin secretion, and energy expenditure simultaneously, potentially offering superior weight loss compared to single-receptor agonists. - What advantages does the dual agonist approach provide?
Dual agonist mechanisms may offer better tolerability and potentially fewer side effects due to more focused receptor targeting, while still providing significant weight loss benefits through synergistic pathways.
Safety Questions
- What are the common side effects of both compounds?
Both compounds share common gastrointestinal side effects typical of GLP-1 receptor agonists, including nausea, vomiting, diarrhoea, and constipation. These effects are generally mild to moderate and tend to diminish over time. - Are there any unique safety concerns with either compound?
Retatrutide may be associated with sleep disturbances and increased heart rate at higher doses. Amycretin has shown generally favourable safety profiles in early studies with no deaths reported. - How do the safety profiles compare?
Both compounds have shown generally favourable safety profiles in early studies, though comprehensive long-term safety data remains limited for both due to their investigational status.
Research Questions
- What are the limitations of comparing these compounds?
Cross-trial comparisons are limited by differences in study design, patient populations, treatment durations, and dosing regimens. The lack of head-to-head trials makes direct comparisons challenging. - What factors should researchers consider when evaluating these compounds?
Researchers must consider study populations, duration of treatment, dose regimens, and the investigational nature of both compounds. Caution is needed when extrapolating findings from clinical trials to broader populations. - How might these compounds fit into future obesity treatment strategies?
Both compounds represent significant advances in obesity pharmacotherapy, offering hope for patients struggling with weight management. Their different mechanisms may allow for personalised treatment approaches based on individual patient needs.
Conclusion
The comparison between Retatrutide and Amycretin highlights the evolving landscape of obesity pharmacotherapy, where different therapeutic strategies offer new hope for patients struggling with weight management. While both compounds target appetite regulation and glucose metabolism, their distinct mechanisms create unique therapeutic profiles with different advantages and limitations.
Retatrutide’s triple agonist approach demonstrates superior weight loss efficacy, with up to 24.2% weight reduction after 48 weeks, positioning it as a leading candidate in the multi-receptor agonist category. The compound’s comprehensive receptor targeting may provide additional metabolic benefits, particularly for patients with type 2 diabetes or metabolic syndrome.
Amycretin’s dual agonist mechanism, while targeting fewer receptors, may offer distinct advantages due to its focused approach and potentially better tolerability profile. The compound has demonstrated impressive weight loss results, with up to 24.3% weight reduction over 36 weeks, suggesting comparable efficacy with potentially better tolerability.
Both compounds represent significant advances beyond single-receptor agonists, addressing multiple aspects of metabolic dysfunction simultaneously. As clinical trials continue and regulatory review progresses, these compounds may transform the treatment landscape for obesity and related metabolic conditions, offering personalised approaches to weight management based on individual patient characteristics and treatment goals.